










{kind=link}
Trent
“Some of the loneliest hours as a physician occur when there is an emergency and it’s just you and the nurse,” says Charles Helm, who recently retired as a practicing physician, though still continues to run the Tumbler Ridge Clinic.
General Practitioners (GPs) regularly face challenging acute medical situations, ranging from what drugs to prescribe to a patient that won’t interact with the drugs that patient is already on, to life threatening injuries.
And while our local physicians hold a vast amount of medical knowledge in their heads, they cannot know everything.
That’s where CODI comes in. CODI stands for Critical Outreach and Diagnostic Intervention and is an iPhone app developed by BC GPs Dr John Pawlovich and Dr Don Burke.
The new app is being rolled out across the north through a partnership between the South Peace Division of Family Practice and Northern Health, and is coming to Tumbler Ridge, Chetwynd and Dawson Creek through a grant from the South Peace Health Services Society.
The CODI app provides rural physicians with instant access to a critical care specialist in real time, 24/7, for support during some of their most stressful and challenging times in the ER, through a video chat-like interface like Skype or Facetime, but encrypted.
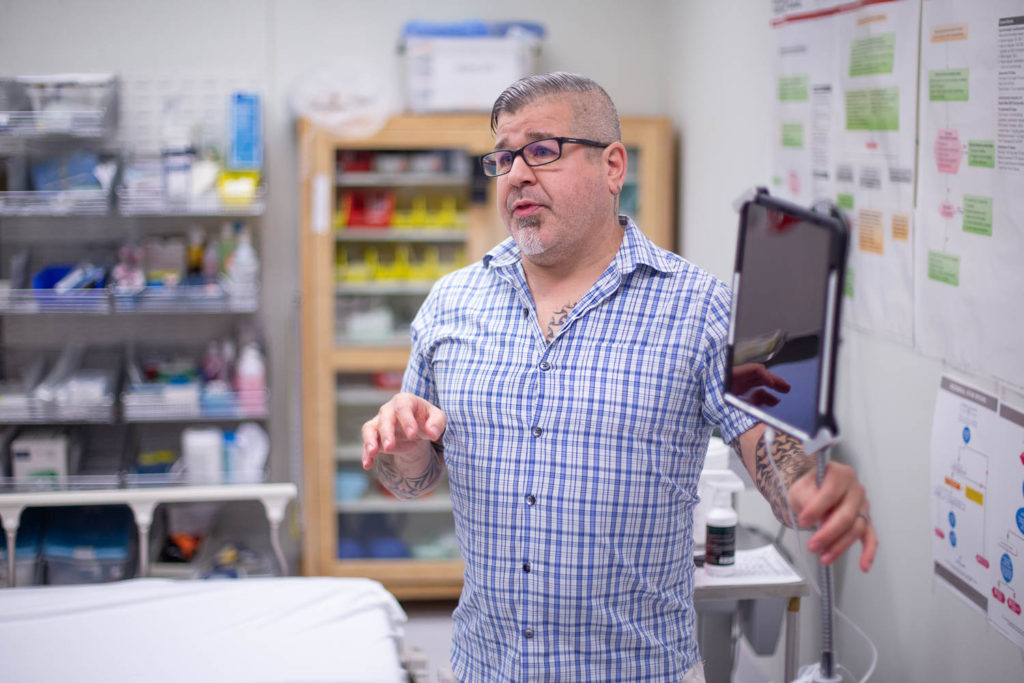
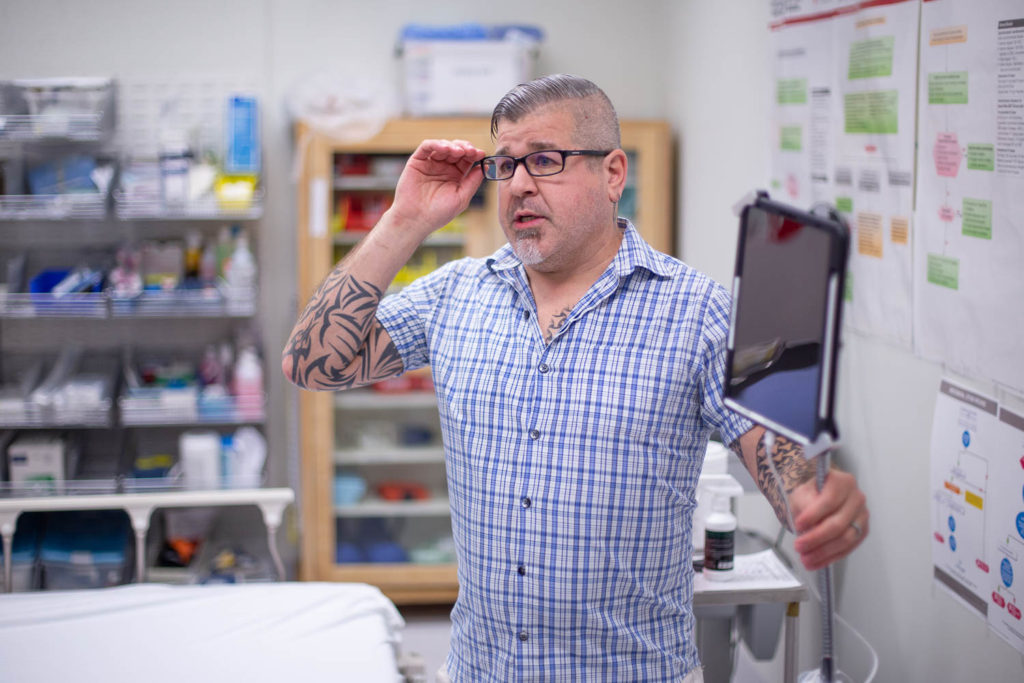
CODI takes the form of an iPad mounted to what looks like an IV stand. The iPad itself is mounted on a goose neck stand, allowing the local physician to move and bend the iPad to show the supporting physician what’s happening, as well as allowing them to operate hands free.
Dave Harris came to town to announce the launch of CODI. He’s the IT Lead for the South Peace Division of Family Practice. He says the CODI app is designed to be easy to use, secure, and user friendly. That last part is important, he says, and not just in it’s technology. The people who are being called need to be professional, courteous and friendly. “I don’t want to be yelled at for feeling inferior for using the app,” he says. “They have to have that empathetic point of view. There is no dumb question. There’s no bad question. There’s no scenario where you shouldn’t call CODI. It is great for emergency situations, but it is also for when you’re in clinic, and you’re dealing with a complex patient, or the patient may not even be there, and you’re trying to sort out medications. And these ICU docs bring a lot to the table.”
Right now, says Harris, there’s a group of seven GPs who man the service, two on at a time. “There was actually one call when the service first went live at one point, and there was a GP that was a little bit short with the rural doctor, and they were right out. That can’t even happen one time. The rural physician has to feel like comfortable to call anytime for this help.”
This service level commitment, says Harris, is the core component of the service. If a call goes to the app and the primary physician on call isn’t able to answer, it goes the second person. If they’re on a call (something Harris says hasn’t happened yet), it will bounce between the two every 30 seconds until it is answered.
This sounds like a long time, but the current service allows physicians to call in and leave a message, and someone will return the call in a few hours.
“A lot of times,” he says, “it’s two in the morning, you have the patient and you have maybe a nurse there, and all four hands are dealing with situation. And you’re very much looking at that situation. You don’t always see the bigger picture, everything else that can be going on. Having this GP in your back pocket, for lack of a better term, they can see the whole thing and help the situation.”
Any advice from the CODI GP shows up as a note in the app, which allows the rural doctor to print the note and attach it to the patient’s chart if they’re being transferred elsewhere.
The app also records the audio of the call, which will allow rural physicians to go back and listen to the details.
A couple of weeks ago, the app was expanded nurse practitioners, nurses and medical residents could use it. “In a lot of First Nations sites and the more northern sites, often times, there will just be a nurse there. And that’s where the need is the greatest. So they should be able to have the access.
There app, says Harris has a lot of potential. “The hope is to expand—for example—to BC ambulance. Let’s say the attendants are maybe 20 minutes out with the patient. They can use the same application to get a hold of the GP that’s sitting in the hospital that’s waiting for them and they can start a consult with full, secure video, they can start that consult while they’re on route, so when they get there, they can hit the ground running.”
There’s also the potential to expand the app to allow GPs to contact specialists, but this adds a level of complexity, says Harris, and they want to make sure they do it right. “Physicians have said loud and clear, they want it to be super simple. Right now, they literally hit the call button, put in the patient number and the patient name. If they don’t have a patient name, there’s a John Doe option. You just hit a button and it starts ringing to them. There’s no filling out forms and all that kind of stuff.”
While a doctor could just use their own phone to call the service, Harris says this allows them to be hands-free. “What we found is initially, when Cody was getting out there, people with their iPhones would be in the ER, and they’d be working and would actually have to call a family member to hold their iPhone over the patient. And that’s really not good. So we came with us hands free device here.”
He says sometimes, the advice is unexpected. “There was a scenario where they were dealing with a person that was on the table. The physician was there, and they were getting ready to bag (a bag valve mask is a hand operated device that allows air to patients that can’t breath properly by squeezing a bag attached to a mask). The CODI GP could see the room, and they could see that there was a ventilator in the back. And they asked, why the rural physicians wasn’t using the ventilator? And the rural physician said, ‘I don’t know how to use it. I wasn’t trained on it. So it’s just sitting in the room doing nothing.’ So the CODI GP told them to bring it over they did a training session and taught the GP how to use the ventilator, and now this GP knows how to use the ventilator in that location. Having that full video option from the intensive is it allows them to actually see the environment and make suggestions when the rural GP may have tunnel vision, dealing with the situation.
The CODI cart costs $2000 with a brand new iPad included. It replaces a telehealth cart with runs in the $35000 range and is a proprietary device. With CODI, a doctor can call in from their own iPhone, using a free app.
CODI was born in BC, but is quickly rolling out across some of the more remote areas of the country, which is exactly who the service is for. And while there are big plans afoot for the app, at the heart is that personal connection. “It’s two in the morning and there’s some anxiety there, and the doctor or nurse needs that person who’s not driving, who can look at the whole cockpit, so to speak, and be like, ‘okay, there’s other stuff going on here. There’s these lights flashing, there’s this, there’s that and the better plan comes up that that’s again, how do we put together a better management plan for the patient for the best outcome possible?’ That’s the driving force.
Mayor Keith Bertrand calls the CODI app “an absolute game changer for our community. Innovative ideas can achieve extraordinary results, and this is certainly an example of that,” he says. “This type of connectivity is paramount for a small community like Tumbler Ridge to become more effective and efficient with the medical service level we can offer here. This is another example of the collaboration within the peace region that will benefit all of our lives.”
Throughout the peace region, mayors, councillors, and area directors have truly made it a priority to try and improve the lives of the residents through improved health care.
“We all have seen and experienced the challenges our medical system encounters every day. But when we can all come together and really bring innovative ideas to reality through collaboration and communication, we can all benefit in some way.”