{kind=link}
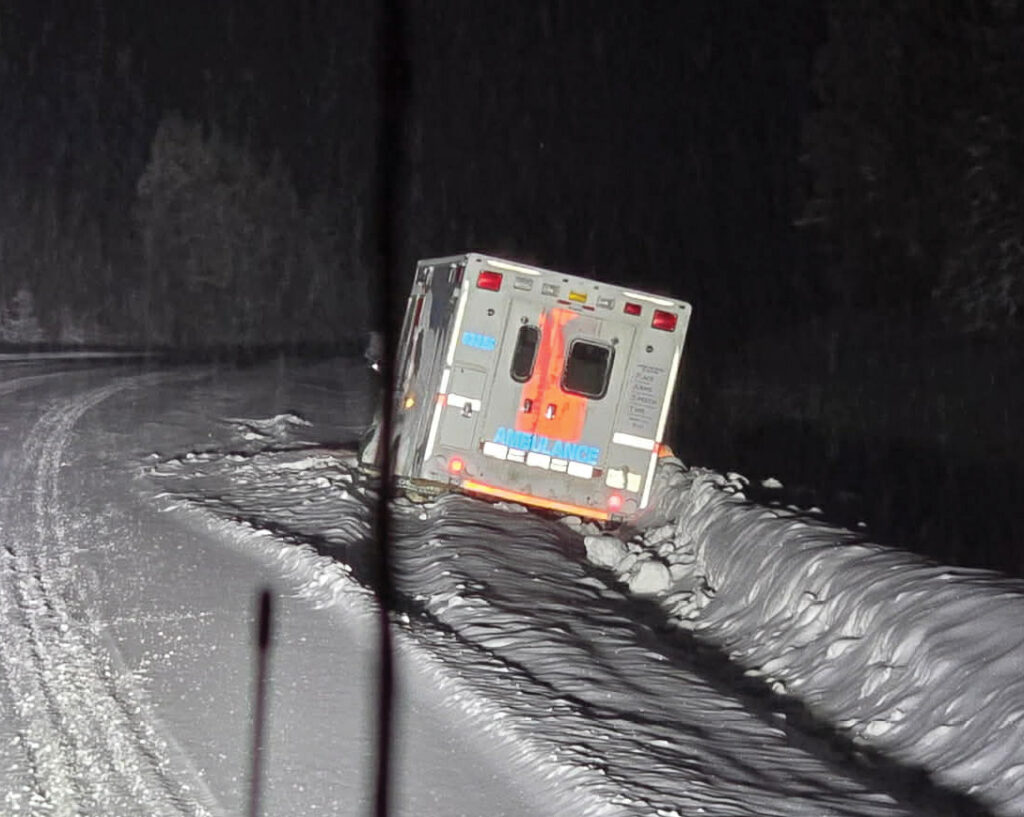
Many of us have now seen the photo on Facebook of one of our ambulances in the ditch on the way to Dawson Creek. (If you haven’t, look right. -editor) Apparently, the transfer occurred on the evening of Saturday January 3.
One’s immediate thoughts go out to the patient being transferred and the ambulance crew, and one hopes that no-one suffered any injuries in this incident. However, it raises further thoughts, which perhaps have not been expressed in the discussion about our now-absent ER services after hours and on weekends. And it provides another example (not that another one is needed) of why this is such a bad direction that our health authority has taken with our health care.
In the good ol’ days, when we had 24/7 ER coverage, those presenting to the ER outside of regular hours could be divided into three categories: some needed to receive treatment and could safely be sent home. Others were seriously ill and definitely needed transfer to a higher level of care. And in between there was a gray zone, where transfer might be worthwhile but might be unnecessary, depending on how one approached the problem. In such situations I and my colleagues would consider other factors at play, such as road conditions. If the roads were dangerous due to the kind of weather we have been experiencing this winter, that would influence our decision, and we could choose to observe the patient for longer, often thus avoiding the need for a transfer. We could always justify such decisions: human lives trump policy any day.
In doing this we were also thinking of the safety of our ambulance personnel. Why burden them with travel on unsafe roads unless it was definitely necessary? When I arrived here in 1992 I was informed by my colleagues of a heart-rending case: the parents of a patient who had been transferred to Dawson Creek were killed in a motor vehicle accident while following the ambulance. My colleagues urged me to be judicious with transfers, and that message stuck with me. I also passed it on to those who succeeded me.
So what happens nowadays? You need medical help after hours, so you call 911. Without seeing a local doctor or a nurse, you are probably going to be transferred to the nearest available option (after someone first checks to see which hospitals may be on diversion). You may be in the category that simply needed local treatment, or you may be in that grey zone and the roads may be bad. Or you may be in the seriously ill zone that definitely needs a transfer after life-saving treatment can be administered locally and your condition can be stabilised. In all these scenarios, you will now be subjected to a long ambulance ride, regardless of which category you fit into. And if you are treated and discharged in the nearest available hospital in the middle of the night, you may not know how to get back to Tumbler Ridge.
In other words, the sensible approach which informed our decision making in the past, providing both patients and ambulance crews with a buffer against unnecessary travel when the road conditions were dismal, is no more. If we believe what our health authority informs us, this is all good for us, as we all need to get to that higher level of care as quickly as possible. Apart from everything else that is wrong with this, it is insulting to our physicians and nurses as it ignores their ability to provide care locally. The photo image of one of ambulances in the ditch is haunting. If our health authority would listen to the lived-experience comments of our residents, and show a willingness to apply the solutions that have been suggested, our health care would be in a very different situation.